Disorders
of Immune System:
Systemic Lupus Erythematosus:
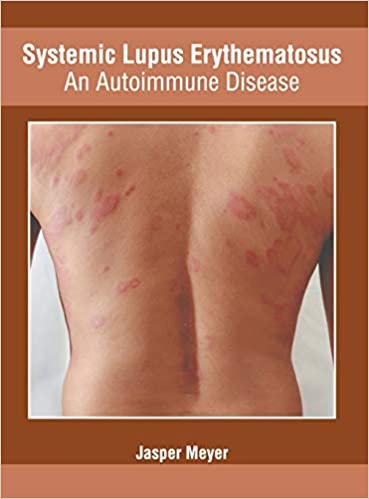
SLE is an autoimmune disease involving multiple organs, characterized by
a vast array of autoantibodies, particularly antinuclear antibodies (ANAs), in
which injury is caused mainly by deposition of immune complexes
and binding of antibodies to various cells and tissues.
Systemic lupus erythematosus (SLE), is the most common type of lupus(Lupus is a systemic autoimmune disease).
The hallmark(distinctive characteristic of something) of SLE is the production of
autoantibodies.
 |
| Systemic Lupus Erythematosus |
Injury(tissue damage) and inflammation to the skin, joints, kidney, and serosal membranes(The serous membrane, or serosal membrane, is a thin membrane that lines the internal body cavities and organs such as the heart, lungs, and abdominal cavity. The thin membrane is made up of mesothelium tissue which originates from the mesoderm) is prominent, but virtually every organ in the body may be affected.
SLE predominantly affects women, with a female-to-male ratio of 9 : 1 for the reproductive age group of 17 to 55 years.
Anti-Nuclear Antibodies:
ANAs can be grouped into four categories:
(1) Antibodies to DNA,
(2) Antibodies to histones,
(3) Antibodies to non-histone proteins bound to RNA, and
(4) Antibodies to nucleolar antigens.
Pathogenesis:
Both genetic and environmental factors play a role in Systemic Lupus Erythematosus
Genetic Factors
*Familial association.
Family members have an increased risk for the development of SLE,
*HLA association.
The odds ratio (relative risk) for persons with HLA-DR2 or HLA-DR3 is 2 to 3, and if both haplotypes are present, the risk is about 5.
*Other Genes.
Genetic deficiencies of classical pathway complement proteins, especially C1q, C2, or C4, are seen in about 10% of patients with SLE. The complement deficiencies may result in defective clearance of immune complexes and apoptotic cells, and failure of B-cell tolerance.
Environmental Factors
Exposure to UV light
UV irradiation(process by which an object is exposed to radiation) may induce apoptosis and also may alter DNA and make it immunogenic.
Gender bias
The gender bias of SLE is partly attributable to actions of sex hormones and partly related to genes on the X chromosome, independent of hormone effects.
Drugs
such as hydralazine, procainamide, and D-penicillamine can induce an SLE-like disorder.
Recent studies in
animal models and patients have revealed several immunologic abnormalities that
collectively may result in the persistent and uncontrolled activation of
self-reactive lymphocytes.
Failure of
self-tolerance in B cells results from defective elimination of self-reactive B
cells in the bone marrow or defects in peripheral tolerance mechanisms.
CD4+ helper
T cells specific for nucleosomal antigens also escape tolerance and contribute
to the production of high-affinity pathogenic autoantibodies.
Mechanisms of Tissue Injury;
Different autoantibodies are the cause of most of the lesions of SLE.
Most of the systemic lesions are caused by immune complexes
(type III hypersensitivity).
DNA-anti-DNA complexes can be detected in the glomeruli and small blood vessels. Low levels of serum complement (secondary to consumption of complement proteins) and granular deposits of complement and immunoglobulins in the glomeruli further support the immune complex nature of the disease. T cell infiltrates are also frequently seen in the kidneys, but the role of these cells in tissue damage is not established.
Autoantibodies of different specificities contribute to the pathology and clinical manifestations of SLE (type II hypersensitivity).
Autoantibodies specific for red blood cells, white blood cells, and platelets opsonize(make more susceptible to phagocytosis) these cells and promote their phagocytosis, resulting in cytopenias(reduction in the number of mature blood cells).
Anti-phospholipid antibody syndrome.
Patients with antiphospholipid antibodies may
develop venous and arterial thromboses, which may be associated with recurrent spontaneous
miscarriages and focal cerebral or ocular ischemia.
This constellation of
clinical features, in association with lupus, is referred to as the secondary
antiphospholipid antibody syndrome.
Morphology
The morphologic changes in SLE are extremely variable.
The most characteristic lesions result from immune complex deposition in blood vessels, kidneys, connective tissue, and skin.
Blood Vessels:
An acute necrotizing vasculitis involving capillaries, small arteries, and arterioles may be present in any tissue. The arteritis leads to fibrinoid necrosis of the vessel walls. In chronic stages, vessels undergo fibrous thickening with luminal narrowing.
Kidney:
Up to 50% of SLE patients have clinically significant renal involvement, and the kidney virtually always shows evidence of abnormality if examined by electron microscopy and immunofluorescence.
Renal involvement takes a number of forms, all of which are associated with the deposition of immune complexes within the glomeruli and shows following lesion pattern.
• Minimal mesangial lupus nephritis
• Mesangial proliferative lupus nephritis
• Focal lupus nephritis
• Diffuse lupus nephritis
• Membranous lupus nephritis
• Advanced sclerosing lupus nephritis
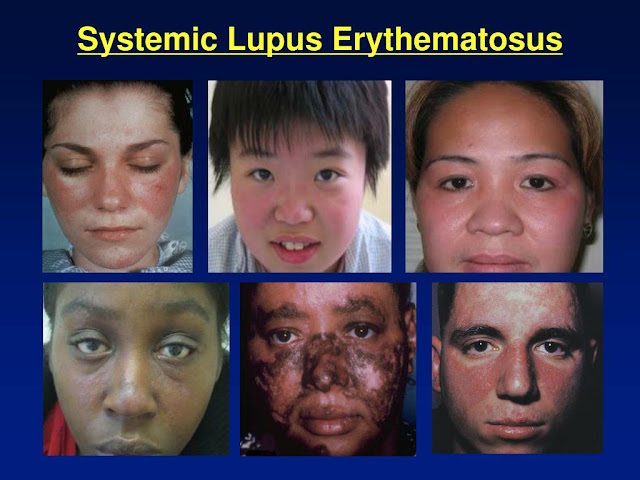
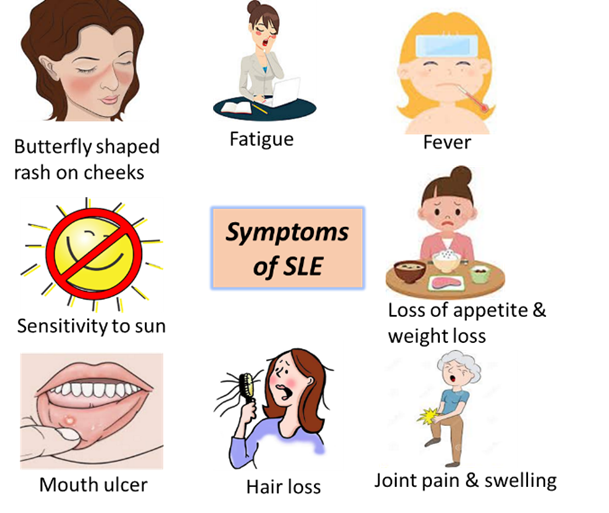
Skin:
Characteristic erythema affects the face along the bridge of the nose and cheeks (the butterfly rash) in approximately 50% of patients, but a similar rash also may be seen on the extremities and trunk. Urticaria, bullae, maculopapular lesions, and ulcerations also occur.
Exposure to sunlight incites or accentuates the erythema. Histologically the involved areas show vacuolar degeneration of the basal layer of the epidermis. In the dermis, there is variable edema and perivascular inflammation. Vasculitis with fibrinoid necrosis may be prominent. Immunofluorescence microscopy shows deposits of immunoglobulin and complement.
Joints
Joint involvement is typically a nonerosive synovitis with little deformity, which contrasts with rheumatoid arthritis.
Central Nervous System
Although it was suggested in the past that the neuropsychiatric manifestations of SLE may be due to acute vasculitis.
Pericarditis and Other Serosal Cavity Involvement:
Inflammation of the serosal lining membranes may be acute, subacute, or chronic. During the acute phase, the mesothelial surfaces are sometimes covered with fibrinous exudate. Later they become thickened, opaque, and coated with shaggy fibrous tissue that may lead to partial or total obliteration of the serosal cavity. Pleural and pericardial effusions may be present.
Cardiovascular system:
Cardiovascular system involvement may manifest as damage to any layer of the heart. Symptomatic or asymptomatic pericardial involvement is present in up to 50% of patients.
Spleen:
Splenomegaly, capsular thickening, and follicular hyperplasia are common features. Central penicilliary arteries may show concentric intimal and smooth muscle cell hyperplasia, producing so-called onion-skin lesions.
Lungs:
In addition to pleuritis and accompanying pleural effusions, some cases are complicated by chronic interstitial fibrosis and secondary pulmonary hypertension.
Other Organs and Tissues. LE, or hematoxylin, bodies in the bone marrow or other organs are strongly indicative of SLE. Lymph nodes may be enlarged due to hyperplasia of B cell follicles or even demonstrate necrotizing lymphadenitis due to vasculitis.












{kind=link}
Social Plugin